Blog 5
A Summary of Nancy’s Journey in MHST601
As a hospital oncology pharmacy manager, my daily work is focused on improving patient care through safe pharmacy practice. My motivation to pursue a Master’s degree in Health Studies at Athabasca University is driven by my professional identity as a health care provider and my growth as a leader in my pharmacy community. My professional identity is shaped by the standards set out by our professional licensing body, the Ontario College of Pharmacists (OCP) and our regulatory body, the National Association of Pharmacy Regulatory Authorities (NAPRA). My role as pharmacy manager leans on an interdisciplinary approach for a complete patient care model which integrates health advocacy with pharmaceutical expertise. My passion for education has brought me into a journey of self-exploration and discovery of who I currently am, and where I intend to go in my personal and professional identity.
The elements that play a critical role in my expertise, are the ability to lead a team and understand my required duties as a pharmacy manager. I have the clinical expertise in chemotherapy regimens, targeted regimens, immunotherapies and supportive care treatments specific to the diagnoses of the patient population we serve in the greater Hamilton, ON area. My educational endeavor has rooted my understanding of pharmacodynamics and pharmacokinetics of oncology medications. My team leadership includes guiding pharmacists, pharmacy technicians and other health professionals in a collaborative and efficient work environment. I have developed strong problem solving skills as a drug information pharmacist and apply them to address complex situations involving medication therapy management, and optimizing outcomes for cancer patients. Patient safety and medication resource allocation is a daily focus of our cancer care team. Part of my manager role is to oversee inventory management, drug costs, staffing budget, regulatory compliance and understand our underserviced minorities to better serve the needs of our community.
In understanding my role as a health care provider, the historical review of the definition of health is valuable. The World Health Organization definition of health “is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity and a fundamental right of every human being without distinction of race, religion, political belief or social condition”. (WHO, 1948). This concept has a foundation in great social equity of the late 1940s. Svalastog brings to light that the WHO definition is missing the additional key component of spiritual health. The individual should have a spiritual self-awareness, self-confidence creating a satisfaction in their life which brings about peace and emotional balance. (Svalastog, 2017). The expanded definition should be inclusive of determinants of health in modern times. Determinants of health are those factors that influence the health of individuals, families and communities. Health Canada (2018) defines determinants of health in the following groups: social, economic and physical environment. Social determinants may be those factors such as, who we value and emulate in our family or community. Social determinants include our culture, coping skills, and childhood experiences. Economic determinants are things such as income, social status, access to health care, quality of health care, healthy behaviors and education level achieved. Physical environment determinants are biology, sexuality, sexual orientation and genetics, including where we live, and where we are employed. These determinants of individuals may lead to health inequities. In oncology determinants of health disproportionately affect marginalized populations, such as Indigenous Canadians. Social, economic and physical environment determinants of health affect our Canadian Indigenous population where a lack of trust for institutional medicine drives health disparities. Abuse, forced separation of aboriginal families are a Canadian history that has had impactful determination on the health care of the lives of indigenous peoples. First Nations Communities, according to Justice Murray Sinclair, feel like they have been burned by mainstream medicine. (Vogel, 2015). Aboriginal women in Canada face a higher rate of breast cancer mortalities due to delayed diagnosis and treatment access barriers. (Cole, 2021).
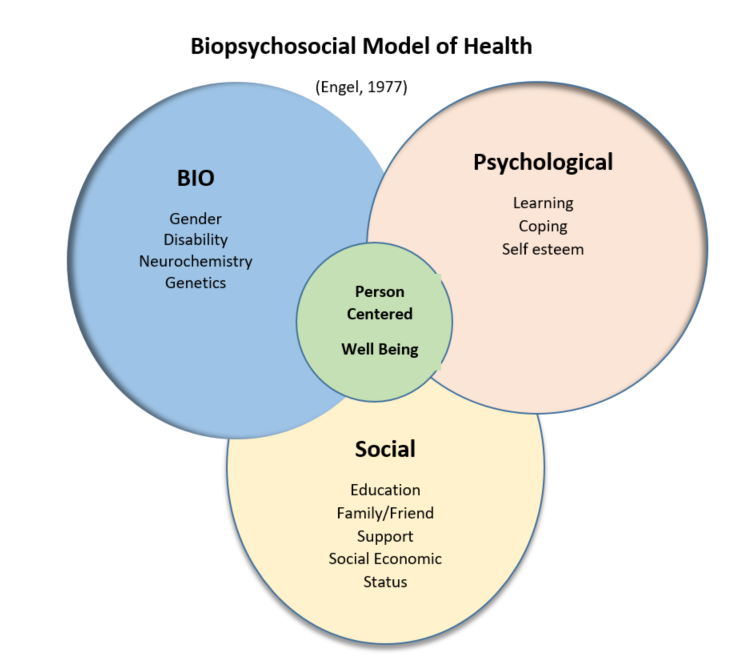
The Biopsychosocial Model of Health by George Engel (1977) places the patient at the centre of the model. Health in this model includes self-determination combined with elements outside of our control. These factors are intertwined together in our lives but can be parsed out to include our genetic predispositions to cancer, late stage diagnosis, the impact of stress, social stigma, lack of mental health support during cancer treatment journey and lack of community support or systemic discrimination of marginalized populations. Multi-spheres influences on health are the elements of social conditions that affect health such as health literacy and coping mechanisms. Study efforts to understand and address social determinants of health show promise for improving health and health equity. (Decamp, 2020). The Biopsychosocial Model when applied to oncology patients supports a better adjustment to their diagnoses if they to have significant others and social networks for their cancer journey. When these factors are missing hopelessness and helplessness are significant mental health outcomes. (Lauriola, 2019). Wade (2017) developed a biopsychosocial model of complexities for a holistic, model of illness. In this context, the person is multi-dimensional entity and complex influences in this model affect the individual and allow them to constantly evolve.
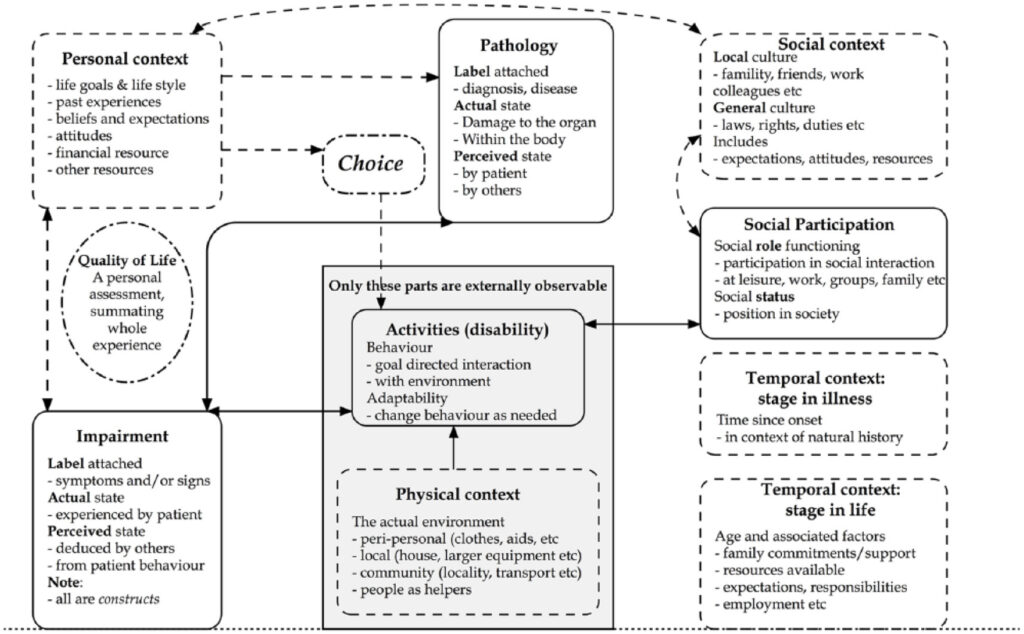
The pathology of illness or disease is part of patient’s social context, social participation and leads to behavioral goals that are impactful on the patient journey and quality of life. One underrepresented group in oncology research that is marginalized are transgender people. Scime, (2019) suggests that cancer care in Canada has limitations related to an absence of large-scale prospective studies among transgender communities and that national registries do not sufficiently report on cancer incidence, prevalence and outcomes. Scime, (2019) further shares that transgender people are five times more likely to be diagnosed with HIV which is associated with higher incidence of cancer primaries such as anal, lung, liver, cervical, Kaposi’s sarcoma and non-Hodgkin’s lymphoma. Leone, (2023) stated that transgender individuals face unique challenges in health care due to barriers in access, discrimination, inequities in treatment that can influence cancer risk and outcomes. Some health care practitioners are not equipped to care for this patient population as professional education programs currently are very limited to curriculum education on transgender and non-binary people. Providing resources such as community organizations, outreach centers, and education allow the broader community and society the ability to support equitable health for all and reducing barriers can improve societal health outcomes. (Decamp, 2020).
Financial funding is a powerful determinant for consideration in cancer care in Canada. As a manager, I am tasked with scrutiny and accountability for the outpatient oncology pharmacy department spend. In Ontario, Cancer Care is provincially funded with programs for cancer treatment for curative and palliative intent.
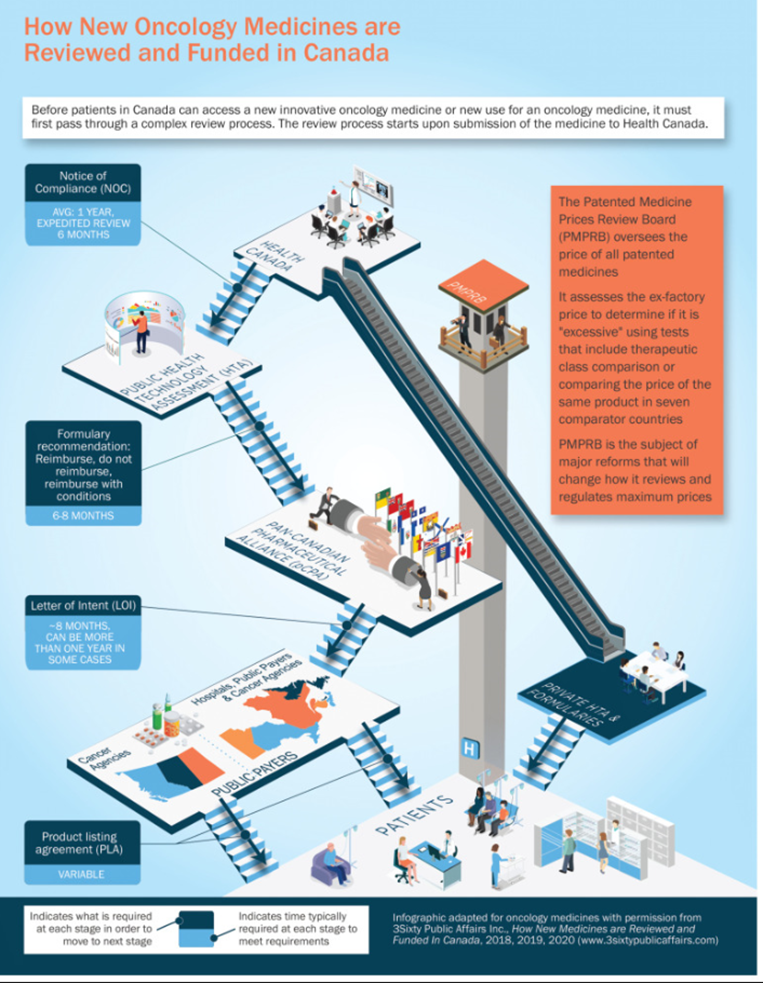
Cancer in general terms can be considered a chronic ongoing illness. Some examples are ovarian cancer, chronic leukemia, lymphomas and metastatic cancers. (Phillips, 2010). Cancer Care Ontario plans to meet their goals for cancer prevention provincially by working with our cancer partners to champion disease prevention, promote chronic disease prevention policies and programs, under take primary, secondary and tertiary prevention and inform disease prevention through research, and population health assessment and surveillance (CCO, 2020). However, there are differences in chronic disease approaches across the nation. Chronic Lymphocytic Leukemia (CLL), is one type of chronic cancer that is linked to increased rates in New Brunswick where the cancer funding and resources differ from Ontario. Provincial attitudes toward cancer screening programs, combined with a lack of provincial government programs or the province’s demographics is impactful on health and health outcomes. (Chowdry, 2022). CLL is the most common leukemia in older adults in North America. CLL is an incurable cancer but is treated with several different drug regimens in targeted therapy and chemo-immunotherapy to prolong life expectancy and palliate with comfort. Tertiary care centres offer treatment which is consistent with best practice guidelines and involved in research, however, for new drug indications, often in Canada, we are behind the USA, in our Health Canada and Cancer Care Ontario approval and funding of drugs in general. (Gotfrit, 2022)
In summary, my journey as a pharmacy oncology manager is continuously evolving. MHST601 Critical Foundations in Health Discipline course has enabled me to realize I am required to emphasize the need for a holistic and equitable approach to oncology care for our patients. There are challenges facing historically marginalized communities, where we need to ensure advocacy and engagement is prioritized. Funding constraints are limitations that require provincial and federal to support and adopt inclusive policies and prioritize the gaps and continue to design education programs that reflect cultural values and the specific needs of our cancer patients with equity across the nation.
References
Canada, H. (2018). Determinants of health – Canada.ca.
Canada.ca. https://www.canada.ca/en/services/health/determinants-
health.html
Chowdhury, N. (Last Updated: August 26 2022). Health experts say
several factors explain N.B.’s high cancer rate. CBC News. https://www.cbc.ca/news/canada/new-brunswick/health-experts-say-several-factors-explain-n-b-high-cancer-rate-1.6562426
Cole, K., Hutton, B., Hamel, C., Bourque, JM., Arnaout, A., & Clemons,
M. (2021). Breast cancer in Indigenous women living in Canada: a
scoping review protocol. JBI Evidence Synthesis 19(12) 3412-
3422. https://journals.lww.com/Fulltext/2021/1200/Breast_Cancer_in_Indigenous_women_living_in.19.aspx
DeCamp, M., DeSalvo, K., & Dzeng, E. (2020). Ethics and spheres of
influence in addressing social determinants of health. Journal of
General Internal Medicine, 35(9), 2743–2745. https://doi.org/10.1007/s11606-020-05973-1
Gotfrit, J., Dempster, W., Chambers, J., & Wheatley-Price, P. (2022).
The pathway for new cancer drug access in Canada. Current Oncology
(Toronto, Ont.), 29(2), 455–464. https://doi.org/10.3390/curroncol29020041
NAPRA.ca – National Association of Pharmacy Regulatory Authorities.
(n.d.). https://www.napra.ca
OCPInfo.com – Ontario College of Pharmacists. (n.d.).
https://www.ocpinfo.com/
Phillips, J. L., & Currow, D. C. (2010). Cancer as a chronic
disease. Collegian Royal College of Nursing, Australia), 17(2),
47–50. https://doi.org/10.1016/j.colegn.2010.04.007
Progress in chronic disease prevention: 2015 to 2020. (2020, May
19). Ccohealth.Ca. https://www.ccohealth.ca/en/what-we-
do/general-health/chronic-
disease-prevention/progress-chronic-disease-prevention-2015-2020
Scime, S. (2019). Inequities in cancer care among transgender people:
Recommendations for change. Revue Canadienne de Nursing
Oncologique [Canadian Oncology Nursing Journal], 29(2), 87–91.
https://canadianoncologynursingjournal.com/index.php/conj/article/view/976/863
Svalastog, A. L., Donev, D., Kristoffersen, N. J., & Gajović, S. (2017). Concepts and
definitions of health and health-related values in the knowledge
landscapes of the digital society. Croatian Medical Journal, 58(6),
431–435. https://doi.org/10.3325/cmj.2017.58.431
The Editors of Encyclopaedia Britannica. (2018). World Health Organization
(WHO) | History, Organization, & Definition of Health. Encyclopedia
Britannica. Retrieved November 29, 2024, from
https://www.britannica.com/topic/World-Health-Organization
Vogel, L. (2014). Broken trust drives native health disparities. Journal de
l’Association Medicale Canadienne [Canadian Medical Association
Journal], 187(1), E9–E10.
https://doi.org/10.1503/cmaj.109-4950
Wade, D. T., & Halligan, P. W. (2017). The biopsychosocial model of illness:
a model whose time has come. Clinical Rehabilitation, 31(8),
995–1004. https://doi.org/10.1177/0269215517709890
Blog 3
Blog 2